Imagine training a heart scan segmentation model with exactly one labeled patient. That is not a hypothetical stress test, it is the actual one percent labeled setting a team from Zhejiang University and Ritsumeikan University put their method through, and the results say something interesting about why simple consistency training sometimes falls apart on medical images specifically.
Key points
- SemSim rebuilds the popular FixMatch weak to strong consistency framework around semantic similarity instead of raw pixel agreement.
- It fixes two blind spots, weak contextual reasoning inside a single unlabeled image and class distribution mismatch between labeled and unlabeled batches.
- On the ACDC cardiac MRI dataset with just one percent labeled data, SemSim reaches a Dice score of 0.872, ahead of the next best method at 0.856.
- A lightweight spatial aware fusion module adds only about 0.79 million parameters yet meaningfully improves segmentation quality.
- The full model still totals only 2.60 million parameters, far smaller than SAM based or diffusion based competitors evaluated in the same paper.
- Results are reported across three very different tasks, cardiac MRI, skin lesion photography, and prostate MRI, which is a reasonable breadth test for a general method.
Why FixMatch alone was not quite enough
Medical image segmentation is one of those tasks where the bottleneck is rarely the algorithm and almost always the labels. Tracing the boundary of a heart chamber slice by slice, or a melanoma lesion pixel by pixel, or a prostate gland through dozens of MRI slices, takes real clinical expertise and real time, and hospitals cannot annotate their entire imaging archive just to train a model. That scarcity is exactly why semi supervised learning keeps showing up in this corner of computer vision.
Among the many semi supervised techniques out there, FixMatch became something of a default choice after it proved itself in image classification. The idea is disarmingly simple. Take an unlabeled image, create a weakly augmented version and a strongly augmented version, let the model’s prediction on the weak version act as a pseudo label, and train the model to match that pseudo label on the strong version, but only when the model is confident enough to trust its own guess. The authors of this paper, Shiao Xie, Hongyi Wang, Ziwei Niu, Hao Sun, Shuyi Ouyang, Yen Wei Chen, and Lanfen Lin, note that this same recipe carries over surprisingly well to medical segmentation benchmarks, especially when labeled data is extremely scarce, which is why they adopt it as their own starting point rather than reinventing the wheel.
But adopting FixMatch as a baseline is not the same as declaring it sufficient, and the paper spends real effort explaining exactly where the simple pixel matching approach breaks down for dense per pixel prediction tasks specifically, as opposed to whole image classification.
Where these ideas came from
Weak to strong consistency and its FixMatch lineage
FixMatch itself was introduced by Sohn and colleagues as a way to simplify semi supervised classification, combining pseudo labeling with consistency regularization and a confidence threshold into one clean training loop. Several follow up works have refined pieces of that recipe. FlexMatch adjusts its confidence threshold dynamically per class based on how well the model is currently learning that class, which cuts training time substantially. FreeMatch adds a self adaptive fairness penalty so the model does not collapse toward predicting only the easiest classes early in training. Fast FixMatch instead focuses on trimming computational cost by scheduling the unlabeled batch size through a fixed curriculum. All of these variants improve some aspect of classification training, but none of them were designed with the specific geometry of dense segmentation labels in mind, which is the gap SemSim tries to close.
Prior semi supervised medical segmentation methods
Segmentation specific semi supervised methods have their own separate lineage. The Mean Teacher framework and its variants push a student network’s predictions toward a slowly updated teacher network’s predictions. BCP Net uses a bidirectional copy paste strategy to blend labeled and unlabeled data directly at the pixel level. CPS trains two differently perturbed segmentation networks and has each one supervise the other with pseudo labels. More recent hybrid approaches bring in Transformers, cross teaching CNN and Transformer branches to capture both local and global dependencies, while still newer entries borrow from diffusion models and from the Segment Anything Model’s prompting mechanism. SemSim positions itself as a return to simplicity, keeping FixMatch as the backbone rather than adding an entirely new generative or foundation model component, while directly addressing the specific failure modes the authors identified.
Two blind spots hiding inside a simple idea
The paper frames its motivation around a classic idea from label propagation research, that features with higher similarity in feature space ought to receive the same label. FixMatch, as originally designed, never explicitly checks for that kind of similarity. It only compares two predictions pixel by pixel. That omission creates two separate problems once you move from classifying a whole image to labeling every pixel in it.
The intra image problem
Inside a single unlabeled image, FixMatch has no mechanism for noticing that two pixels belonging to the same anatomical structure, say two neighboring points inside the same heart chamber, should be treated as related. Without that contextual reasoning, the model’s predictions can become locally inconsistent, producing segmentation masks with gaps, holes, or fragmented regions instead of one coherent structure. The paper illustrates this with class activation map visualizations showing FixMatch producing discontinuous, incomplete activation for a given anatomical class where SemSim produces a more unified region.
The cross image problem
The second blind spot sits between images rather than inside one. Labeled and unlabeled data are assumed to come from the same underlying class distribution, but when there is only a handful of labeled examples, ordinary supervised training on just those examples does not fully capture that distribution, and a gap opens up between how the model represents a class using labeled data versus how it represents that same class when it encounters unlabeled data. The paper backs this up with kernel density estimates of feature values for the myocardium class in the ACDC dataset, showing FixMatch’s labeled and unlabeled distributions visibly diverging while SemSim’s stay much closer together.
Relying solely on the existing pixel wise consistency constraint from FixMatch is not sufficient for medical segmentation. Both problems trace back to the same root cause, a method that only checks whether two predictions agree, without ever asking whether the underlying features that produced those predictions are actually similar to each other.
How SemSim actually closes both gaps
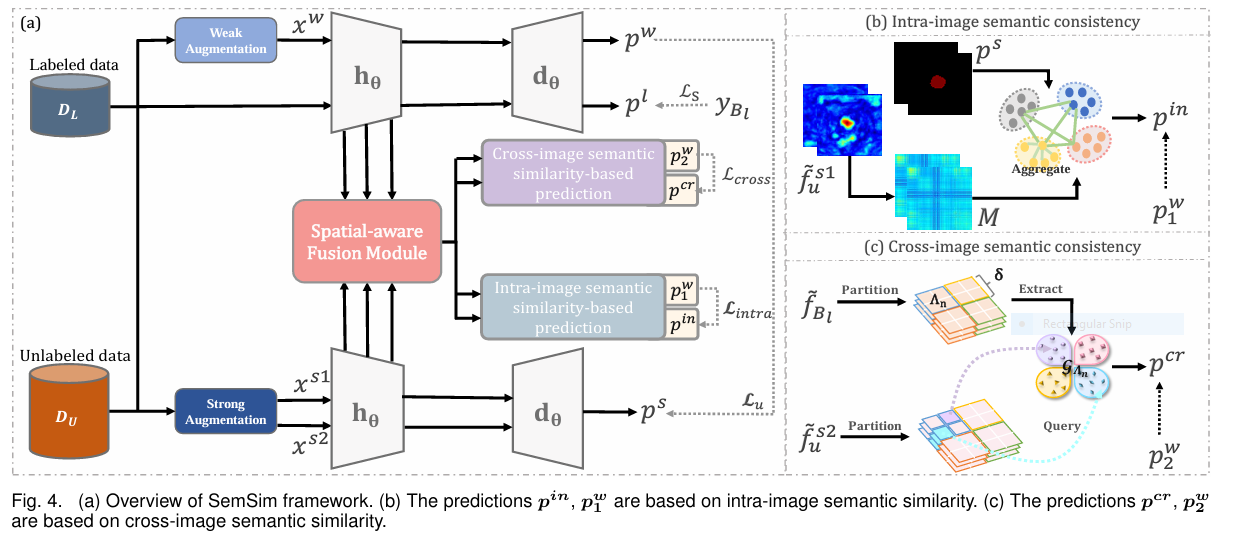
Rather than feeding a single strongly augmented view into the network the way FixMatch does, SemSim generates two independent strongly augmented views of each unlabeled image, alongside the usual weakly augmented view. Each of the two strong views feeds a different consistency mechanism, one aimed at the intra image problem and one aimed at the cross image problem, and both mechanisms sit on top of the same encoder and decoder used for ordinary segmentation.
Intra image semantic consistency, reasoning with an affinity map
For the first strongly augmented view, the encoder’s multi scale features get passed through a fusion module described below, producing an enhanced feature map. That feature map is reshaped and used to compute a pairwise affinity map, essentially a similarity score between every pair of pixel locations in the feature map, using a cosine style normalized dot product followed by a softmax. Because this affinity map captures which pixels in the image are semantically alike, the original per pixel segmentation prediction gets refined by mixing in these pairwise relationships, producing what the paper calls an intra image semantic similarity based prediction. That refined prediction is then compared, in the usual weak to strong consistency fashion, against the model’s prediction on the weakly augmented view, giving an explicit training signal that rewards contextual coherence rather than only isolated pixel agreement.
Cross image semantic consistency, querying the labeled batch
The second strongly augmented view feeds a different mechanism entirely. Instead of comparing an unlabeled image only to itself, SemSim builds a set of class prototypes from the labeled batch in the same training step, then asks the unlabeled image’s features to query those prototypes directly. A naive version of this idea would average all labeled features of a given class into one single global prototype, but the authors point out that medical image backgrounds contain wildly different anatomical structures depending on where in the image you look, so one global average per class would blur that structure away. Instead, SemSim partitions each labeled feature map into small sub regions and computes a separate local prototype for each class within each sub region. An unlabeled image’s features are compared against the prototypes from the matching sub region using cosine similarity, and the resulting similarity scores get turned into a cross image semantic similarity based prediction through a softmax style normalization.
Weighing the cross image signal by its own uncertainty
Early in training, a network’s features are still unreliable, so directly trusting a cross image prediction from day one would be risky. SemSim adds an uncertainty estimate specifically for this purpose, computed by comparing each labeled image’s similarity map against the batch averaged similarity map using a KL divergence style calculation. Predictions that diverge a lot from the batch average get treated as more uncertain, and that per pixel uncertainty score directly scales down the cross image consistency loss wherever the model does not yet seem to know what it is doing.
The original FixMatch unsupervised loss compares the weak and strong predictions directly, filtered by a confidence threshold.
$$L_u = \frac{1}{|B_u|} \sum \mathbb{1}(\max(p^w) \geq \tau) \odot L_{dice}(p^w, p^s)$$SemSim adds an intra image loss between the weak prediction and the affinity refined prediction.
$$L_{intra} = \frac{1}{|B_u|} \sum \mathbb{1}(\max(p_1^w) \geq \tau) \odot L_{dice}(p_1^w, p^{in})$$And a cross image loss, scaled by the uncertainty term, between the weak prediction and the prototype queried prediction.
$$L_{cross} = \frac{1}{|B_u|} \sum \mathbb{1}(\max(p_2^w) \geq \tau) \odot L_{ce}(p_2^w, p^{cr}) \odot \bar{U}$$The three unsupervised terms combine, then average with the supervised loss for the final training objective.
$$\tilde{L}_u = \lambda L_u + \lambda_{intra} L_{intra} + \lambda_{cross} L_{cross}, \quad L = \frac{1}{2}(L_s + \tilde{L}_u)$$The spatial aware fusion module behind the scenes
Both the intra image affinity map and the cross image prototype matching depend entirely on having good features to begin with, so the authors built a dedicated fusion module to strengthen the feature maps feeding into both mechanisms. Multi scale features are well known to help with objects that vary a lot in size, but naively concatenating tokens from every scale into one long sequence and running a standard Transformer block over it gets computationally expensive fast.
Instead, the spatial aware fusion module works in three steps. Patch matching lines up corresponding patches across three neighboring scales that share the same spatial location, flattens and concatenates them, and keeps the sequence short by only comparing genuinely related patches rather than the entire feature map at once. Scale interacting then runs multi head self attention and a small feed forward block over just those matched patch groups. Scale splitting reshapes the enhanced sequence back into per scale feature maps, which get interpolated to a common resolution and fused through a convolution layer. The authors work out the computational complexity explicitly, showing their windowed approach costs roughly the full sequence complexity divided by the square of the window size, a meaningful saving over processing every scale’s tokens together in one giant attention operation.
Training setup and hyperparameters
SemSim uses a standard UNet as its encoder decoder backbone, with all input slices resized to 224 by 224. Strong augmentation combines color transformation with CutMix, while weak augmentation is simply random flipping, matching the setup used by an earlier cross teaching baseline the authors compare against. Training runs for 300 epochs with SGD, a weight decay of one times ten to the negative fourth, momentum of 0.9, an initial learning rate of 0.01, and a batch size of 16 split evenly between labeled and unlabeled samples. A channel dropout of 50 percent probability is added as an extra feature level perturbation. The fused feature channel dimension is set to 128, the uncertainty scaling hyperparameter r is set to 1000, and the confidence threshold tau is set to 0.95, a notably strict bar for trusting a pseudo label. The three loss weights, lambda for the base FixMatch term, lambda intra, and lambda cross, are set to 0.5, 0.25, and 0.25 respectively, based on a sensitivity sweep the authors ran and reported in their hyperparameter analysis.
What the experiments actually show
SemSim gets evaluated against twenty other semi supervised methods across three genuinely different medical imaging tasks, which is a broader test than many segmentation papers attempt. The ACDC dataset covers cardiac MRI with three structures, the right ventricle, myocardium, and left ventricle, split across 70 training, 10 validation, and 20 test patients, evaluated at 1 percent, 5 percent, and 10 percent labeled ratios corresponding to 1, 3, and 7 labeled cases. The ISIC dataset is a two class skin lesion segmentation task built from 1838 training and 756 validation images, evaluated at 3 percent and 10 percent labeled ratios. The PROMISE12 dataset covers prostate MRI segmentation from 50 patients split into 35 training, 5 validation, and 10 test cases, evaluated at 3 percent and 7 percent labeled ratios.
| Dataset | Labeled ratio | Best prior method | Best prior DSC | SemSim DSC | SemSim other metric |
|---|---|---|---|---|---|
| ACDC cardiac MRI | 1 percent | CPC SAM | 0.856 | 0.872 | 95HD 1.8mm |
| ACDC cardiac MRI | 5 percent | CPC SAM | 0.880 | 0.888 | 95HD 1.9mm |
| ACDC cardiac MRI | 10 percent | CPC SAM | 0.890 | 0.896 | 95HD 2.3mm |
| ISIC skin lesion | 3 percent | BCP Net | 0.769 | 0.774 | 95HD 18.9mm |
| ISIC skin lesion | 10 percent | BCP Net | 0.794 | 0.802 | 95HD 13.3mm |
| PROMISE12 prostate MRI | 3 percent | MedFCT | 0.725 | 0.758 | ASSD 1.6mm |
| PROMISE12 prostate MRI | 7 percent | BCP Net | 0.772 | 0.784 | ASSD 1.3mm |
A few things stand out reading these numbers side by side. The margin over the previous best method is largest exactly where labeled data is scarcest, which is arguably the scenario that matters most in practice, since fully labeled datasets rarely need semi supervised tricks in the first place. On ACDC at 1 percent labeled, SemSim’s Dice score of 0.872 comes with a boundary distance of only 1.8 millimeters, a meaningfully tighter boundary fit than most competing methods report at that same labeled ratio, several of which the paper notes were too unstable to report reliably below 0.3 Dice under 1 percent labeling. On PROMISE12, the gains over training with labeled data alone are dramatic, roughly plus 20 percentage points of Dice, which says a lot about how much unlabeled prostate MRI data there was for the model to draw on relative to the tiny labeled fraction.
Parameter efficiency is another point the authors highlight directly. The full SemSim model totals only 2.60 million parameters, compared to 19.37 million for DiffRect and a much larger 93.75 million for CPC SAM, both of which SemSim outperforms or matches on ACDC. A stripped down variant without the spatial aware fusion module, which the paper calls SemSim minus, still beats every other listed method while using only 1.81 million parameters, which tells you the intra and cross image consistency losses are doing most of the actual work, and the fusion module is squeezing out an additional, smaller gain on top.
Relying solely on existing consistency constraint is far from sufficient for medical image segmentation. Summarized position from Xie, Wang, Niu, Sun, Ouyang, Chen, and Lin, arXiv:2410.13486
What the ablation studies reveal
The authors ran a careful ablation on ACDC at 1 percent labeled to isolate what each piece of the loss function actually contributes. Using only the intra image consistency loss already beats the plain FixMatch baseline. Using only the cross image consistency loss alone also beats the baseline, though by a smaller margin. Combining both losses together produces a bigger jump than either alone, roughly 1.7 and 3.7 percentage point improvements over using just one of the two, which the authors read as evidence that the two mechanisms are addressing genuinely different failure modes rather than duplicating each other’s effect. Adding the original FixMatch consistency term back in alongside both new losses gives the final reported result, a Dice score of 0.872 with a 95 percent Hausdorff distance of only 1.8 millimeters.
A separate ablation on the number of feature sub regions used for cross image prototype matching found a sweet spot at four sub regions across all three datasets. Fewer sub regions blur too much anatomical detail into each prototype, while more sub regions shrink each region so much that there is not enough data inside it to build a reliable class prototype, and performance drops in both directions. The spatial aware fusion module was also tested at different network stages, and fusing features from stages two, three, and four together gave the best tradeoff, while including the very shallowest stage actually hurt performance and added unnecessary computational cost.
The clinical translation gap
It is worth being direct about the distance between these numbers and an actual clinical workflow. All three datasets used here are established public research benchmarks with fixed, curated splits, not the messy variability of scanners, protocols, and patient populations a hospital would encounter across sites. The ACDC dataset covers only 100 patients total, the PROMISE12 dataset only 50, and the ISIC evaluation split, while larger in image count, still represents a specific curated collection of dermoscopic images rather than the full range of real world skin photography conditions, lighting, and camera types a deployed screening tool would face.
The paper also does not report any comparison against inter observer variability among human clinicians, which is normally how you would judge whether an automated segmentation’s disagreements with one expert annotator fall inside the ordinary range of disagreement between two experts. Nor does it break results down by specific pathology subtypes, disease severity, or patient demographics within each dataset, so it is not possible to know from this paper alone whether performance holds up evenly across harder clinical presentations, such as an unusually shaped heart chamber after cardiac remodeling or an atypical, irregularly bordered melanoma.
None of this takes away from the technical result. It does mean a strong Dice score on ACDC, ISIC, or PROMISE12 is evidence of a promising research method, not a demonstrated readiness for use in patient care, and the authors frame their contribution accordingly as a methods paper rather than a clinical validation study.
Where this could go next
The three ideas at the center of SemSim, an intra image affinity map, cross image prototype querying with sub region partitioning, and an efficient cross scale fusion block, are not tied to any one imaging modality. The same semantic similarity framing could plausibly extend to other dense prediction tasks facing the same core constraint, a handful of expensive expert labeled scans next to a much larger unlabeled pool, which describes plenty of radiology and pathology problems beyond the three datasets tested here. The authors also leave open how their sub region prototype scheme would behave on fully 3D volumes rather than 2D slices, since all three benchmarks here were processed as 2D slices even where the underlying scan is a 3D volume.
Honest limitations
A handful of limitations deserve attention beyond what the clinical translation section already covers. The labeled sample sizes across all three benchmarks are genuinely small in absolute terms, one to seven labeled cardiac patients, 55 to 181 labeled skin lesion images, and roughly one to three labeled prostate patients depending on the exact split, which means even a well designed method is being asked to generalize from a very thin slice of real world variation. The paper’s own results table flags that several competing methods became too unstable to report meaningfully below a 0.3 Dice score at the 1 percent labeled setting, which is a useful reminder of just how difficult this regime is for the field generally, SemSim included, even though it clearly handles it better than the alternatives tested.
As a preprint rather than a peer reviewed journal publication at the time of writing, and as a paper reporting purely technical segmentation metrics rather than any clinical outcome or diagnostic accuracy study, its results should be read as a meaningful methodological advance on established public benchmarks, not as evidence that the system is ready to inform an actual diagnosis or treatment decision.
Read the source material
The full derivations, all twenty method comparisons, and every ablation table are available directly from the authors.
A complete PyTorch implementation of the core ideas
What follows is a runnable, simplified reimplementation of SemSim’s three consistency losses and its fusion module, written for clarity rather than to match every detail of a production nnU-Net style pipeline. It uses a small UNet backbone so the whole thing can run a smoke test on dummy data without a GPU, while keeping the affinity map computation, the sub region prototype querying, the uncertainty weighting, and the windowed cross scale fusion logically faithful to the paper’s equations.
Bringing it together
The core achievement of this paper is a fairly narrow, well aimed fix rather than a wholesale replacement of the FixMatch recipe. The authors kept the weak to strong consistency backbone that already worked reasonably well for medical segmentation, and instead of discarding it, they diagnosed precisely where it was leaving performance on the table, inside a single image where context gets ignored, and across the labeled and unlabeled split where class distributions quietly drift apart. Both fixes plug directly into the existing pipeline rather than requiring a new architecture from scratch.
There is a genuine conceptual shift buried in how the cross image mechanism is built, too. Instead of the common approach of computing one global prototype per class, the authors recognized that medical image backgrounds are spatially heterogeneous in a way natural images often are not, and building local, sub region specific prototypes turned out to matter enough to show up clearly in their ablation results. That is a detail specific to how anatomy is organized in medical scans, and it is exactly the kind of domain informed design choice that separates a method built for medical imaging from one merely borrowed from general computer vision.
The breadth of the evaluation also deserves credit. Testing across cardiac MRI, skin lesion photography, and prostate MRI, three modalities with very different appearance statistics, gives more confidence that the intra and cross image consistency ideas generalize as a principle rather than being tuned to one dataset’s quirks. The consistent margin over twenty competing methods across all three, especially in the most severely labeled scarce settings, is a meaningful result by that standard.
At the same time, the honest limitations matter just as much as the headline numbers. Every benchmark here still represents a curated, fixed research split rather than the messy diversity of real clinical deployment, the absolute labeled sample counts remain small even in relative terms, and the paper reports no comparison against human inter observer variability, which is the yardstick that would actually tell you whether SemSim’s remaining errors fall inside or outside the normal range of disagreement between two trained clinicians.
Taken as a whole, SemSim reads as a carefully reasoned argument that semantic similarity, not just raw prediction agreement, is the missing ingredient in weak to strong consistency training for segmentation, backed by a lightweight implementation and results that hold up across three genuinely different medical imaging problems rather than just one.
Frequently asked questions
What is SemSim in plain terms?
SemSim is a semi supervised medical image segmentation framework built by researchers from Zhejiang University and Ritsumeikan University. It starts from the FixMatch weak to strong consistency idea and adds two new consistency losses based on semantic similarity, one that looks for relationships between pixels inside a single unlabeled image, and one that compares unlabeled images against labeled data across the whole training batch.
What two problems does SemSim fix in FixMatch?
The paper identifies an intra image problem, where FixMatch ignores contextual relationships between pixels inside one image and produces incomplete or fragmented segmentation, and a cross image problem, where the class distribution learned from a small labeled set drifts away from the distribution the model encounters in unlabeled data.
How well does SemSim perform with very little labeled data?
On the ACDC cardiac MRI dataset with only 1 percent labeled data, which corresponds to a single labeled patient, SemSim reaches a Dice score of 0.872 with a 95 percent Hausdorff distance of 1.8 millimeters, ahead of the next best reported method at a Dice score of 0.856, according to the paper’s own comparison table.
What is the spatial aware fusion module for?
It is a lightweight Transformer based module that combines features from multiple scales efficiently, using a windowed patch matching strategy instead of running full self attention over every token at every scale. It adds about 0.79 million parameters on top of the base model and provides a further, smaller performance gain beyond what the two new consistency losses already deliver.
Is SemSim ready for use in an actual hospital or clinic?
No. This is a research method evaluated on three public academic benchmarks with curated, fixed splits. It has not undergone clinical validation, regulatory review, or testing across the range of scanners, imaging protocols, and patient populations a real deployment would require. Any question about an actual cardiac scan, skin lesion, or prostate MRI finding should go to a licensed physician or radiologist.
How big is the SemSim model compared to other recent methods?
The full SemSim model uses only 2.60 million parameters, considerably smaller than DiffRect’s 19.37 million or CPC SAM’s 93.75 million parameters, while still matching or beating both on the ACDC benchmark according to the paper’s reported comparison table.
Academic citation. Xie, S., Wang, H., Niu, Z., Sun, H., Ouyang, S., Chen, Y. W., and Lin, L. SemSim, Revisiting Weak to Strong Consistency From a Semantic Similarity Perspective for Semi Supervised Medical Image Segmentation. arXiv:2410.13486, 2024.
This analysis is based on the published paper and an independent evaluation of its claims.
Pingback: CMKD: Slash 99% Storage Costs & Dominate UDA Challenges - aitrendblend.com