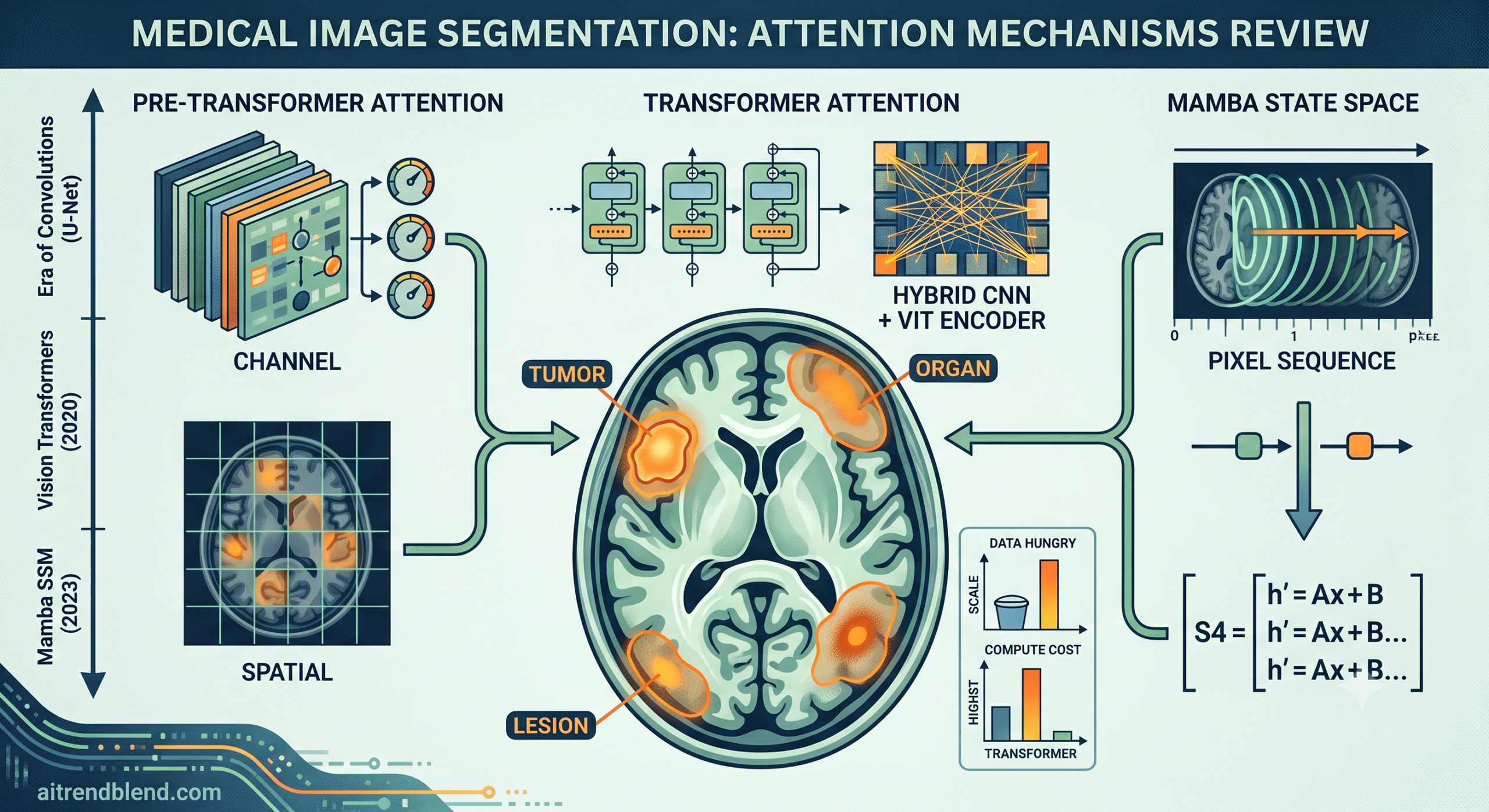
- The review sorts roughly two hundred papers into three families, attention methods built before transformers, transformer based attention, and the newer Mamba style state space methods.
- Channel and spatial attention, the pre transformer tools, are cheap to run and easy to interpret, but their narrow receptive field struggles with large or scattered anatomical structures.
- Transformer attention captures relationships across an entire image, which is why almost every recent architecture pairs it with a convolutional network rather than replacing convolutions outright.
- Mamba based state space models promise transformer level context modeling at close to linear computational cost, and early results on organs, tumors, and polyps look competitive.
- The authors are candid that the field lacks task specific attention design, standardized benchmarks, and almost any published analysis of when these models fail.
The problem that no single trick has solved
Segmenting a medical image sounds simple until you try it. The boundary between a tumor and healthy tissue is often blurry rather than crisp, because soft tissue does not offer the kind of contrast a natural photograph does. The same organ can look different in size, shape, and position from one patient to the next, so a model trained on one hospital’s scanner settings can stumble on another. And labeled data is expensive. Drawing a pixel accurate outline around a liver tumor takes a trained radiologist real time, and that time is scarce and costly. The review frames these three constraints, poor contrast, anatomical variability, and scarce annotation, as the reason attention mechanisms became so central to the field rather than a passing trend.
Attention, in the neural network sense, borrows an idea from human vision. When you scan a room looking for your keys, you do not process every square inch with equal effort. Your visual system assigns more weight to plausible locations and less to the ceiling or the wall. A segmentation network that does the same thing, assigning higher weight to voxels that look like tumor tissue and lower weight to background, tends to draw cleaner boundaries with less training data than a network that treats every pixel identically.
Here \(g(x)\) generates the attention weights from the input, and \(f\) applies those weights back onto the input \(x\), which is the general form the review uses to describe every attention variant that follows.
Background. Three eras, one shared idea
The paper organizes its two hundred references into a timeline that maps neatly onto the broader history of computer vision. Convolutional networks such as U-Net, introduced by Olaf Ronneberger’s group and now the default starting point for almost every medical segmentation project, dominated the field through the late 2010s. Attention arrived first as a small add on inside these convolutional networks. Then, following the debut of the Vision Transformer in 2020, transformer style self attention took over as the fashionable upgrade. Most recently, state space models built around the Mamba architecture from 2023 have started showing up in segmentation papers, promising the context modeling of a transformer without the same computational bill.
What is worth noticing, and what the review keeps circling back to, is that none of these eras fully replaced the one before it. Pure transformer models still lean on convolutional patch embedding to turn an image into a sequence. Pure Mamba models still borrow convolutional stems for the same reason. The field has not found a way to escape convolution entirely, it has found new ways to combine it with longer range context modeling.
Channel, spatial, and temporal attention before transformers
Before transformers, three flavors of attention did almost all the work. Channel attention, popularized by squeeze and excitation networks from Jie Hu and colleagues in 2018, treats each feature channel as if it represents a distinct kind of object and reweights channels based on how useful they are for the task. Spatial attention, exemplified by the attention gate from Ozan Oktay’s team, instead highlights specific regions of an image, suppressing background and sharpening focus on organs or lesions. Temporal attention shows up mainly in video based tasks such as tracking a surgical instrument across frames of an endoscopy recording.
These mechanisms get slotted into a network in one of four places, the encoder, the decoder, the skip connections that bridge the two, or some hybrid combination of all three. The review notes an interesting pattern here. Several independent groups found that placing attention in the decoder, closer to where the final segmentation map is produced, tends to outperform placing it purely in the encoder, possibly because encoder features are still too abstract and generic to benefit as much from selective weighting. That is a genuinely practical takeaway for anyone designing a new architecture, not something you would guess from the abstract of any single paper in the citation list.
The transformer takeover
Self attention, the mechanism behind the transformer, computes a weighted relationship between every pair of positions in a sequence rather than only nearby ones. Applied to an image cut into patches, this lets a model relate a pixel in the top left corner to one in the bottom right corner directly, something a convolution with a small kernel simply cannot do without stacking many layers.
Each of the \(h\) attention heads learns to focus on a different kind of relationship in the image, and the results are concatenated and projected back through \(W^O\) into a single representation, following the original transformer formulation from Ashish Vaswani and colleagues.
The catch is that self attention has no built in sense of locality. A convolution assumes that nearby pixels are related, which is a genuinely useful assumption for images and one that self attention has to learn from scratch. Combined with the fact that transformers tend to need large labeled datasets to reach their potential, and medical datasets are almost always small by natural image standards, this is why the review finds that hybrid designs pairing convolutional encoders with transformer blocks vastly outnumber pure transformer architectures in medical segmentation. TransUNet, one of the earliest and still most cited examples, drops a transformer into the bottleneck of a standard U-Net and reported strong gains on abdominal organ segmentation. Later work such as CoTr, UNETR, and Swin UNETR pushed the idea further, placing transformer blocks at multiple stages or replacing the entire encoder with a transformer while keeping a convolutional decoder.
Mamba and the return of efficient sequence modeling
State space models are not new. They come from control theory, where a hidden state evolves over time according to a small set of matrices. The 2022 Structured State Space Sequence model, known as S4, showed that this old idea could be adapted for deep learning and could model very long sequences efficiently. The core equations look like this.
The state matrix \(\mathbf{A}\) and the projection matrices \(\mathbf{B}\) and \(\mathbf{C}\) map an input signal \(x(t)\) through a hidden state \(h(t)\) to an output \(y(t)\). Once discretized for deep learning, the same relationship can be computed as a convolution using a structured kernel \(\mathbf{K} = (\mathbf{CB}, \mathbf{CAB}, \ldots, \mathbf{CA}^{L-1}\mathbf{B})\), where \(y = x * \mathbf{K}\).
Albert Gu and Tri Dao’s Mamba, released in 2023, made one crucial change. Earlier state space models used fixed parameters for every position in a sequence, which limits how well they can reason about which parts of the input actually matter. Mamba lets its projection matrices depend on the input itself through what the authors call a selective scan, so the model can dynamically decide what to remember and what to forget as it moves through a sequence. That selectivity is computed with a hardware aware parallel algorithm, which is why Mamba can match transformer style performance while scaling roughly linearly with sequence length instead of quadratically.
Applying this to images required another adaptation, since a picture does not have the same left to right ordering as a sentence. Vision Mamba, introduced by Lianghui Zhu and colleagues, scans an image forward and backward to capture context from both directions. VMamba goes further with a four way cross scanning pattern called SS2D, sweeping the image from all four corners so that every pixel eventually sees context from the entire frame. In medical segmentation specifically, SegMamba was the first design built for three dimensional volumes, U-Mamba paired Mamba blocks with residual convolutional blocks inside a U-Net style shell, and VM-UNet became the first architecture to use Mamba blocks as the backbone for both the encoder and the decoder.
How the numbers stack up across the three families
The review does not run a single unified benchmark, since the underlying papers were tested on different datasets under different protocols, which is itself one of the paper’s honest criticisms of the field. What it does provide is a structured comparison of strengths and typical use cases, summarized here.
| Attention family | Typical strength | Main limitation | Where it tends to be placed | Representative models |
|---|---|---|---|---|
| Pre transformer, channel and spatial | Cheap to train, interpretable, works with limited labeled data | Narrow receptive field, struggles with large scale or scattered structures | Encoder bottleneck, decoder, skip connections | Squeeze and excitation networks, attention gate, CBAM, DANet |
| Transformer based | Full image context, strong on structures with complex inter organ relationships | High compute cost, needs large annotated datasets, weak built in locality bias | Encoder bottleneck, dual path encoder, full encoder and decoder | TransUNet, CoTr, UNETR, Swin UNETR, nnFormer |
| Mamba based state space | Transformer level context at close to linear compute cost | Still an early field with limited maturity, longer training times reported in several papers | Hybrid encoder, pure encoder with convolutional decoder, full encoder and decoder | SegMamba, U-Mamba, VM-UNet, Mamba-UNet, Swin-UMamba |
A second table worth pulling out covers where each family shows up most often in the clinical literature the review surveyed, which matters if you are trying to figure out whether a given approach has actually been tested on your organ of interest.
| Clinical task | Common benchmark dataset | Attention pattern most reported |
|---|---|---|
| Brain tumor segmentation | BraTS multimodal benchmark | Squeeze and excitation blocks in the decoder, more recently multi branch transformer or Mamba fusion across MRI modalities |
| Abdominal multiple organ segmentation | BCV dataset | Hybrid encoder with convolutional decoder for two dimensional slices, transformer encoder and decoder for full three dimensional volumes |
| Cardiac segmentation | ACDC dataset | Spatial attention tuned to subtle cardiac borders, used for both segmentation and downstream diagnosis |
| Polyp segmentation | Kvasir-SEG, CVC-ClinicDB, CVC-ColonDB | Spatial attention on high level features, pyramid vision transformer style encoders, progressive decoders |
| Skin lesion segmentation | HAM10000, ISIC2018 | Spatial attention placed in skip connections to handle varying lesion size and shape |
The clinical translation gap
Here is where it gets interesting, and where the review’s honesty is genuinely valuable. Almost every number quoted across those two hundred papers comes from a public, retrospective, single institution benchmark such as BraTS, ACDC, BCV, Kvasir-SEG, or ISIC2018. These are useful for comparing algorithms against each other, but they are not the same thing as a model performing well inside an actual hospital workflow with scanners from different manufacturers, patient populations the model has never seen, and clinicians who need to trust and act on the output under time pressure.
None of the architectures described in this review have gone through the kind of prospective, multi site clinical validation that would be needed before a regulator or a hospital procurement committee would treat them as decision support tools rather than research prototypes. The review itself does not claim otherwise, its scope is squarely academic benchmarking, and it says so directly when it calls for standardized, publicly accessible datasets that better capture the true diversity of medical imaging data. That gap between a strong Dice score on BraTS and a tool a radiologist can rely on during a real case is the single biggest thing separating this body of research from clinical use.
There is also an interpretability angle that matters clinically even though the review treats it mainly as a technical detail. Attention maps are often presented as a way to see what the model is focusing on, which sounds like it should help a clinician trust or double check a prediction. But the review’s own section on failure cases notes that there is almost no published research on what happens when those attention maps are wrong, meaning a clinician has limited grounds for knowing when to trust the visualization and when to override it.
What practitioners can actually do with this
If you are choosing an architecture for a new segmentation project rather than reading this purely out of curiosity, the review’s material maps onto a fairly practical decision tree. If your dataset is small, your labels are expensive, and your task involves a well defined organ with a fairly consistent shape, a pre transformer approach such as an attention gated U-Net remains a sensible and cheap starting point. If you have a moderate amount of data, need to capture relationships between structures spread across a large field of view such as multiple abdominal organs, and have access to reasonable compute, a hybrid convolutional and transformer encoder is the well tested middle ground. If you are working with large three dimensional volumes, need long range context, and have the compute budget to match, a pure transformer or a Mamba based encoder and decoder is worth serious consideration, keeping in mind that the Mamba ecosystem is younger and has fewer battle tested implementations to borrow from.
One thing the review is refreshingly blunt about is that most existing attention designs are generic rather than tuned to the anatomy or pathology at hand. A lung nodule and a liver tumor are different problems with different scale distributions and different surrounding tissue, yet most published attention modules are applied to both without modification. The authors call this out directly as an open research gap, and it is a reasonable thing for anyone building a production pipeline to keep in mind, since a module that performed well on one organ in a paper may not transfer as cleanly as the benchmark tables suggest.
Honest limitations of this body of research
It is worth being direct about what this review can and cannot tell you. First, the comparisons across the roughly two hundred papers are not apples to apples. Different studies use different train and test splits, different preprocessing, and different evaluation metrics, so a higher reported Dice score in one paper does not automatically mean a better method than a lower score in another. The authors flag this lack of standardization as one of their top priorities for future work rather than glossing over it.
Second, most of the Mamba based methods surveyed have only been tested on two dimensional slices rather than full three dimensional volumes, even though many of the clinical tasks involved, brain tumors, liver tumors, cardiac structures, are inherently three dimensional. That limits how confidently the reported gains generalize to volumetric clinical data.
Third, and this is the gap that matters most for anyone thinking about deployment, the review found essentially no published research analyzing failure cases, meaning the specific situations where an attention mechanism focuses on the wrong region and produces an incorrect segmentation. Without that kind of analysis, it is hard to know the practical failure modes a clinical team would need to guard against.
Finally, this is a review of existing published work rather than a new clinical study with its own patient cohort, so there is no new sample size, no new confidence interval, and no new prospective outcome data to report here beyond what each of the roughly two hundred cited papers already published in their own retrospective, public benchmark settings.
Where this leaves the field
The problem runs deeper than picking the fashionable architecture of the year. Each of the three families this review covers solves a real constraint. Pre transformer attention solves the small data problem. Transformer attention solves the limited receptive field problem. Mamba based attention is trying to solve the compute cost problem that comes with wanting transformer level context everywhere. None of the three has made the other two obsolete, and the review’s own closing sections predict that hybrid designs combining convolution, transformer, and Mamba components are the most likely direction for the next generation of medical segmentation networks, rather than any one family winning outright.
The authors also point toward multi modality and multi task learning as an underexplored direction, noting examples such as a federated split vision transformer that co trains segmentation, classification, and detection for COVID-19 diagnosis, and the widely discussed Segment Anything Model being adapted for medical imaging with mixed results depending on modality. Both point toward a future where segmentation is one output among several from a shared backbone rather than a standalone task, which would change how these architectures get evaluated and deployed.
Conclusion
Strip away the acronyms and this review is really about a single tradeoff that keeps reappearing across three generations of methods, how much global context a model can capture against how much data and compute it needs to capture it well. Pre transformer channel and spatial attention answered that tradeoff conservatively, staying cheap and interpretable at the cost of a narrow field of view. Transformers answered it aggressively, buying global context with heavy compute and an appetite for labeled data that medical imaging rarely supplies in abundance. Mamba based state space models are the field’s latest attempt to have both, transformer level reach at closer to convolutional cost, and the early results collected in this survey suggest that attempt is working well enough to take seriously.
The conceptual shift worth remembering is that attention stopped being a bolt on trick sometime around the arrival of the Vision Transformer and became a structural design decision, one that shapes where an architecture places its encoder, its decoder, and its skip connections rather than something added as an afterthought inside an existing convolutional block. That shift shows up clearly in how the review organizes its own taxonomy, moving from what to use, to how to use it, to where it gets applied, a framework that itself reflects how much more deliberate architecture design has become since squeeze and excitation networks first popularized channel attention in 2018.
The ideas here are not locked to medical imaging either. The same attention families driving tumor and organ segmentation are the ones reshaping natural image segmentation, video understanding, and increasingly robotics perception, so progress in one domain tends to migrate quickly into the others. Anyone tracking vision transformers or state space models generally will recognize most of the building blocks in this review even if they never touch a medical dataset.
What is missing, and the authors are candid about this, is task specific design tuned to the anatomy at hand, standardized benchmarks that allow fair comparison across papers, and above all a serious look at when and how these models fail. Those gaps matter more than another incremental Dice score improvement, because they are the gaps standing between an impressive benchmark result and a tool a hospital would actually trust.
For now, the honest summary is that attention mechanisms have made medical image segmentation measurably better on public benchmarks, and the field is still working out how to responsibly bridge the distance between that benchmark performance and the messier, more variable reality of clinical practice. That bridge, more than any new architecture, looks like the next real milestone.
Read the full peer reviewed survey covering all two hundred papers, taxonomies, and benchmark tables.
Read the paper on Computer Science ReviewFrequently asked questions
What is an attention mechanism in medical image segmentation
It is a component inside a neural network that learns to assign higher weight to image regions that matter for the task, such as a tumor or an organ boundary, and lower weight to background, which tends to improve segmentation accuracy especially when training data is limited.
What is the difference between channel attention and spatial attention
Channel attention reweights entire feature channels, treating each one as representing a different learned concept. Spatial attention instead reweights specific locations within an image, highlighting relevant regions such as a lesion and suppressing irrelevant background.
Why did transformers become popular for medical image segmentation
Transformers use self attention to relate every position in an image to every other position directly, which captures long range context that convolutional networks struggle to model without stacking many layers. Because pure transformers need large labeled datasets, most medical designs pair them with convolutional layers instead of replacing convolutions outright.
What is Mamba and why is it showing up in medical imaging papers
Mamba is a state space model architecture introduced in 2023 that models long sequences with a selective scan mechanism, giving it context modeling ability close to a transformer while scaling more efficiently with sequence length. In medical segmentation this translates into designs such as SegMamba, U-Mamba, and VM-UNet that aim for transformer level accuracy at lower computational cost.
Are any of these AI segmentation models approved for clinical use
The review covers academic research and public benchmark results. It does not describe any of the surveyed models as cleared or approved medical devices, and using such a model for actual patient diagnosis or treatment would require separate regulatory review and clinical validation beyond what is reported in this research literature.
Which attention approach should a small research team start with
For a small labeled dataset and a well defined single organ or lesion, a pre transformer approach such as an attention gated U-Net is usually the most practical starting point, since it is cheap to train and does not require the large data volumes that transformer or Mamba based encoders tend to benefit from.
Related reading
This analysis is based on the published paper and an independent evaluation of its claims.
Pingback: Sam2Rad: Transforming Medical Image Segmentation with AI